

By Stephy Wenjun Xiong
From 2011 to 2015, USAID spent nearly 2.5 billion dollars, in an effort to improve health performance worldwide. These interventions focus on specific efforts such as Family Planning and Reproductive Health, HIV/AIDS, Maternal and Child Health, Tuberculosis, Water Supply and Sanitation, Malaria, Pandemic Influenza and Other Public Health Threats.
Despite a large decrease in the global burden of these two infectious diseases during the recent 5 years, malaria and tuberculosis have remained among the top 10 causes of death in low-income countries. (1) They are both communicable diseases and are curable and preventable. Between 2010 and 2015, the incidence of the two infectious diseases decreased globally due to high awareness and effective interventions and treatments. Many international organizations have provided financial support for countries with a high burden.
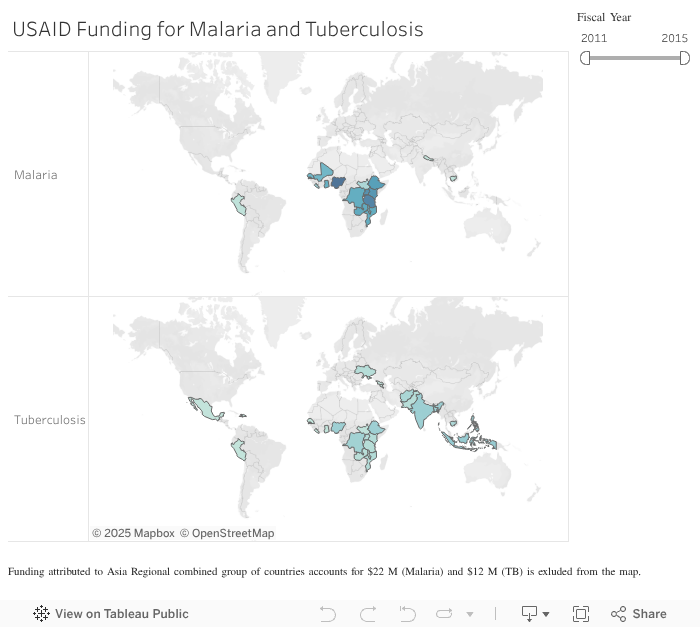
The USAID Dollars to Results dataset shows that most of the funding from USAID for malaria was spent in Africa. This may be due to the fact that the African region contained 90% of the global burden of malaria cases and 92% of malaria deaths in 2015. (2) Nigeria, marked as dark blue, has received the most money compared to other countries, with a total of 239 million dollars aid in 5 years. Tanzania received about 203.5 million dollars.
Compared to malaria, USAID spent less money on tuberculosis programs. Some Asian countries have high burden of tuberculosis, including India, Indonesia and China. These three countries, along with Nigeria, Pakistan and South Africa account for 60% of the new tuberculosis cases in 2015(3). From 2011 to 2015, Indonesia and India received the greatest amount of aid from USAID, totaling 109.5 million dollars.
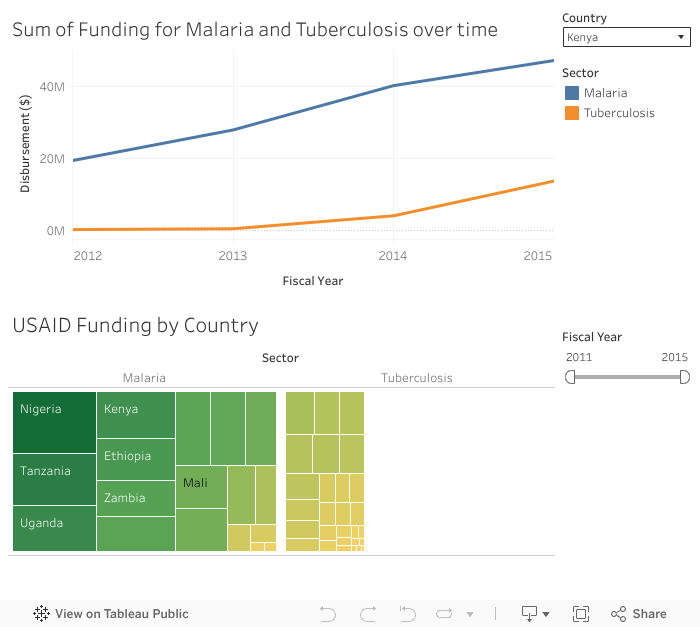
Over time, international support for malaria and tuberculosis has increased steadily. From 2013 to 2014, USAID strengthened its efforts to engage in malaria programs. The disbursement increased from 309.6 million (2011) to 505.6 million dollars (2015). The majority of malaria efforts include bilateral activities, primarily through the U.S. President’s Malaria Initiative (PMI). The U.S. connects with more than 30 countries bilaterally with PMI. (4) With this support, the number of insecticide treated nets distributed in Nigeria increased from 614,000 (2011) to 9,019,215 (2015). Similar trends can be seen with USAID-sponsored tuberculosis interventions. Since 2006, USAID has supported tuberculosis control and prevention in the Asia-Pacific region. Although the amount of aid was limited from 2011 to 2015 compared to malaria programs, the aid supported low- and middle-income countries to access medicine and treatment.
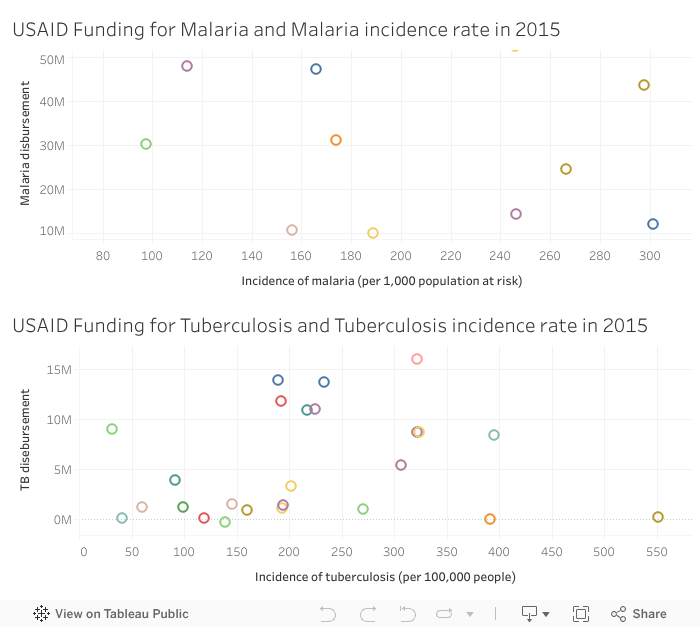
When we compared the USAID 2015 funding with the World Bank dataset of disease incidence, we can have an image of the effect of malaria and tuberculosis programs. For malaria, Ethiopia, Tanzania, Kenya and Uganda had a relatively lower incidence rate with a high amount of aid. Mali and Rwanda were two countries with high burden but received less support. For tuberculosis, Zambia and Mozambique had high incidence combined with minimal funding.